CAPD+

CAPD is not a treatment you go to — it is a treatment you carry with you. Continuous Ambulatory Peritoneal Dialysis means four fluid exchanges a day, every day, at home, managed by the patient alone. For someone with end-stage kidney failure, this procedure is not a medical appointment. It is their life.
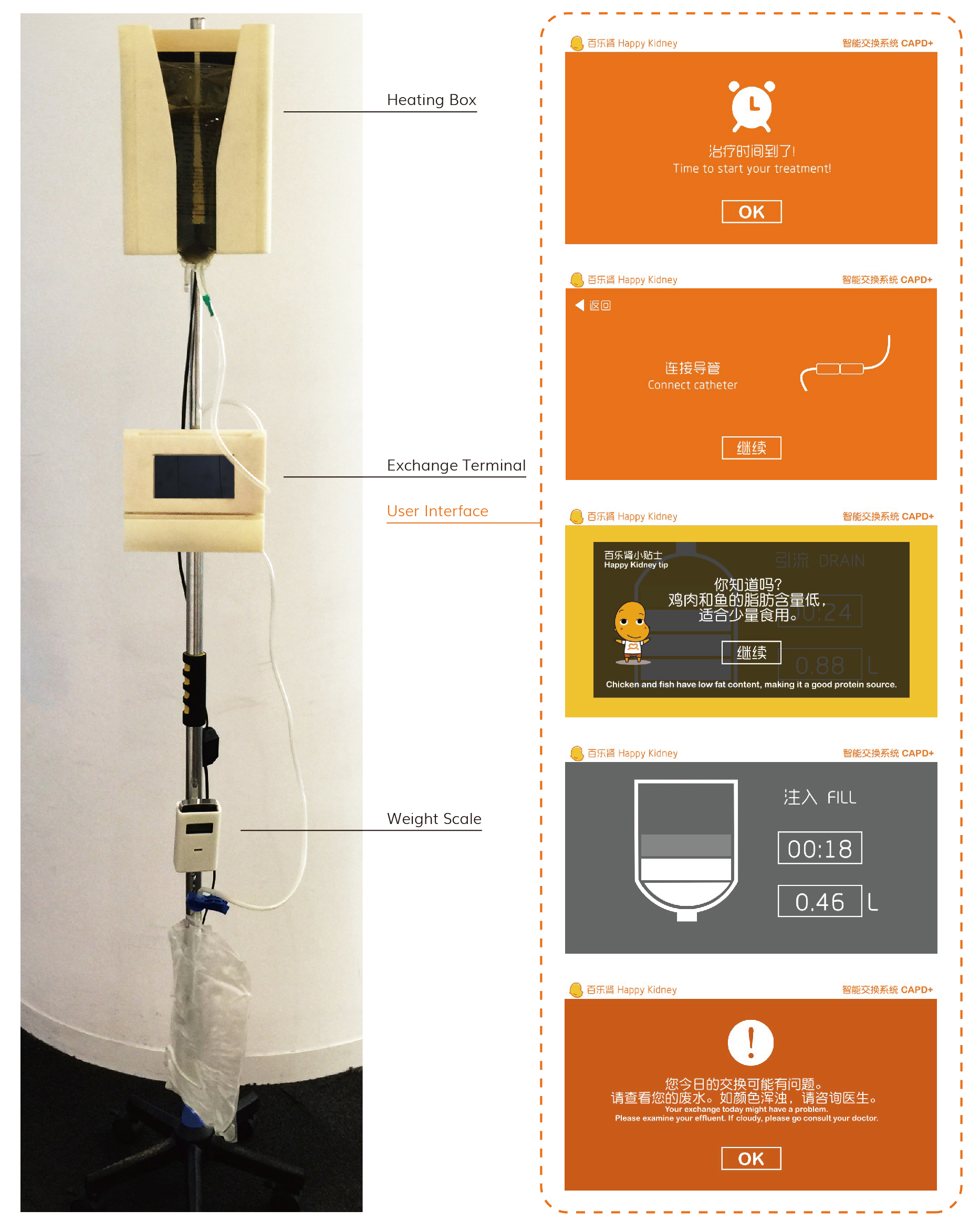
During my internship at Baxter Healthcare in Shanghai, we were asked to look at this experience from the patient's perspective — and to ask whether design could make it better. The project produced hardware and software prototypes: how might a next-generation CAPD device be held, operated, and connected? What would a supporting application need to offer in terms of guidance, feedback, and reassurance for someone performing a clinical procedure at the kitchen table, alone, twice before noon?
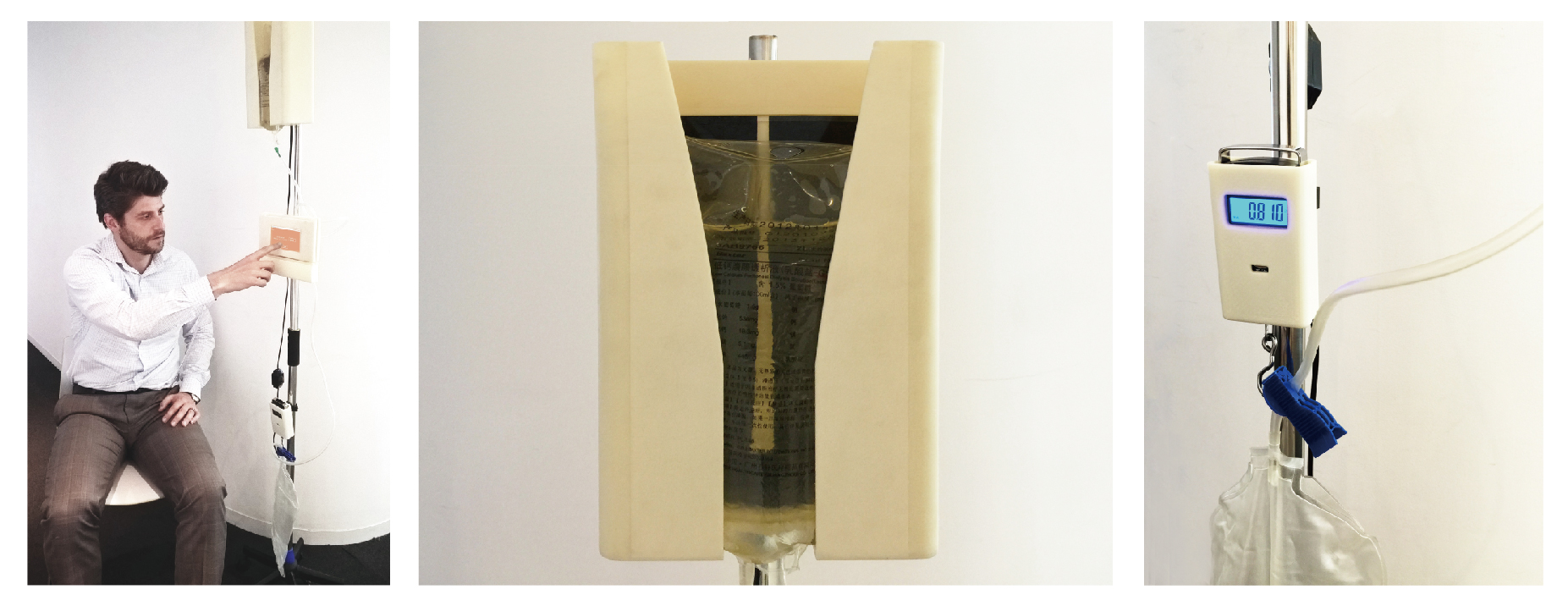
What I did not expect was the testing. Sitting with real patients — watching them interact with what we had made, where they hesitated, what they understood without instruction, what made the procedure feel fractionally more manageable — changed something in how I understood this work. Design, in most contexts, is an exercise in the conditional: we imagine users, we model behaviour, we predict. Here there was no imagining. The people in the room had catheters in their abdomens and came back to this table every day.
I left this internship knowing, with a clarity I had not had before, that I wanted to work at this intersection of design and medicine. Not because healthcare is a prestigious field to be in, but because I had seen what careful, considered design can actually do for a person. The small things — how a connector feels under uncertain fingers, how a screen communicates during a tiring routine — can matter enormously to someone for whom this is not a product experience but a daily act of survival.
CAPD+ is where I became a medical designer. The work itself is student work, and I see its limits clearly now. But the direction it pointed in has not changed.